今天推荐的是《Intensive Care Medicine》上刊登的Ricci等作者的《对急性肾损伤(AKI)的10大错误理解》。
The 10 false beliefs in adult critical care nephrology.
Ricci, Zaccaria., Romagnoli, Stefano., Ronco, Claudio.. (2017). ,
Intensive Care Med 2017 Dec 01
影响因子:12.015
PMID:29196792
DOI:10.1007/s00134-017-5011-x
https://link.springer.com/article/10.1007%2Fs00134-017-5011-x
-
误解:急性肾小管坏死是AKI的主要组织病理学改变(Acute tubular necrosis is the main histopathologic fnding in AKI)
作为一种在缺血性损伤后观察到的组织学模式,急性肾小管坏死(ATN)被认为是任何形式的急性肾损伤(AKI)的最常见原因,尽管这缺乏广泛的组织学证据。这种想法源自既往在创伤患者活组织检查中观察到的ATN结果。 然而,ATN在AKI中并不常见(图1),并且在长时间的热缺血和再灌注过程中,它不能准确地反映形态学变化。 在大多数情况下,危重病人的AKI是脓毒症和大手术的并发症。 在这种情况下,ATN并不常见(有限与散发的),而大量实验证明有其他病理生理学的非缺血性机制参与其中。
Acute tubular necrosis (ATN), a histological pattern observed after ischemic insult, is considered the most frequent cause of any form of acute kidney injury (AKI) despite the absence of extensive histological data. Tis belief derives from previous observations of ATN in biopsies of trauma patients. ATN is, however, uncommon in AKI (Fig. 1) and it does not accurately refect the morphological changes during prolonged warm ischemia followed by reperfusion [1]. In the majority of cases, AKI in the critically ill patient is a complication of sepsis and major surgery. In such cases, ATN is uncommon (limited and sparse) and other pathophysiological non-ischemic mechanisms are involved as suggested by a lot of experimental data.
-
误解:急肾脏血流减少是脓毒症发生AKI的主导原因(Decreased renal blood fow is the leading cause of AKI during sepsis)
肾脏灌注不足被认为通过肾缺氧机制导致脓毒症AKI的主要原因之一,尽管肾血流(RBF)难以在人体内进行研究,但来自高动力性脓毒症动物模型的数据显示AKI是在RBF增加和肾传导性(肾血管舒张)减少的框架下发生的。人类脓毒症的可用数据是有限的,往往是不可靠的,在许多情况下,脓毒症的RBF与肾功能不相关。 高动力性脓毒症时RBF的增加与脓毒性AKI中ATN的缺乏相匹配。 另外,甚至在RBF增加的情况下,包括氧分流、毛细血管密度下降的微循环功能障碍,以及可能对肾小管细胞产生毒性效应的炎症介质浸润(细胞因子、趋化因子、补体)均可导致肾功能障碍。Renal hypoperfusion is considered one of the leading causes of AKI in sepsis via a mechanism of renal hypoxia but, although renal blood fow (RBF) is diffcult to investigate in humans, data from animal models of hyperdynamic sepsis have shown that AKI occurs in the context of increased RBF and a reduction of renal conductance (renal vasodilatation). Available data in human sepsis are limited and often unreliable and, in many cases, RBF during sepsis does not correlate with renal function [5]. The increased RBF during hyperdynamic sepsis matches well with the paucity of ATN in septic AKI. In addition, microcirculatory dysfunction, including convective shunting of oxygen and decrease in capillary density, and fltration of infammatory mediators (cytokines, chemokines, complement fragments) which may exert toxic effects on tubular cells, may contribute e to renal dysfunction even in case of increased RBF.
-
误解:急少尿患者需液体冲击试验(Fluid challenge is always recommended in patients with oliguria)
这段太长,我就简译了:
既往将继发于肾脏灌注不足导致肾衰的原因归于“肾前性”,但如今这样的理解存在很大的偏差。实际上,肾脏的低灌注既可以继发于因心脏前负荷不足所致的肾动脉血流不足(例如低血容量),也可继发于心功能不全(例如心衰),这两种情况均以肾灌注不足为特点,但显然截然不同——一个是输液有反应,另一个则无!此外,对于CVP已增加的扩张性心衰或右心衰,补液可因全身静脉充血(充血性肾衰)而损害肾功能。若存在充血,补液试验以及液体正平衡也是肾功能障碍的预测因子。因此,在补液之前应根据个体情况调整,CVP或可帮助医生进一步了解静脉(充血)对AKI的影响。一句话,补液试验并非“放诸四海而皆准”的单一考查AKI的反应标准。
……one is fuid responsive [increase of cardiac output after fuid loading, for which central venous pressure (CVP) is a poor predictor] while the other is not. On the contrary, fuids administered in conditions where the CVP is increased, such as diastolic heart failure or right ventricular failure, are likely to compromise renal function through systemic venous congestion (congestive kidney failure). When congestion is present, fuid loading and positive fuid balance are predictors of kidney dysfunction compromising the transrenal pressure gradient [8]. Tus, treatment should be adjusted to individual conditions prior to start fuid administration and CVP may help the clinician to suspect the venous contribution to AKI. A fuid bolus should not represent the single “one size fts all” response to AKI

-
误解:急平均动脉压(MAP)是AKI患者血流动力学管理的基准目标(Mean arterial pressure is the principal hemodynamic target in patients with AKI)
尽管大量的随机试验建议脓毒性休克患者复苏以平均动脉压(MAP)为65 mmHg 为目标以保证器官灌注,但几乎没有证据表明MAP能充分代表肾灌注。 已经证实,就灌注压而言,以舒张期动脉压(DAP) – CVP计算的舒张灌注压(DPP)与AKI的发展相关。低DAP,高CVP和低平均灌注压(MPP = MAP – CVP)与脓毒性AKI相关,而MAP无此关系。 CVP升高和/或DAP降低似乎是肾功能障碍的关键决定因素。 而且,DAP的改变被认为与血管张力的改变相关。 有鉴于此,由于DAP降低与AKI有关,因此可考虑使用血管加压药预防/治疗。
Despite large randomized trials suggesting to target mean arterial pressure (MAP) of 65 mmHg after fuid resuscitation in patients with septic shock [9] in order to guarantee organ perfusion pressure, there is little evidence that MAP adequately represents kidney perfusion. It has been demonstrated that, in terms of perfusion pressure, diastolic perfusion pressure (DPP), calculated as diastolic arterial pressure (DAP) − CVP, is associated with the development of AKI. Low DAP, high CVP, and low mean perfusion pressure (MPP = MAP − CVP) were associated with septic AKI while MAP was not. Elevation of CVP, and/or decrease in DAP, seems to be a key determinant of kidney dysfunction. Moreover, the change in DAP is believed to correlate with alteration of vascular tone. In this light, since decreased DAP is associated with AKI, vasopressors may be considered for its prevention/treatment.
-
误解:急AKI后肌酐水平的恢复代表着肾脏的完全康复(Creatinine level restoration after AKI implies full renal recovery)
根据KDIGO标准,从AKI完全康复通常被定义为血清肌酸酐(sCr)恢复至低于AKI的阈值。这个概念存在严重的局限性,因需要对基础Scr鉴别以明确因既往慢性肾病而不可恢复的部分。用急性起病之前的近期sCr或用公式进行反算可能是不准确的。入住ICU的SCr经常被容量复苏的稀释作用所改变。受到药物影响后肌酐自肾小管的排泌可能导致高估肾小球滤过率。 最重要的是,SCr受肌肉量和蛋白质摄入量,肝脏疾病和横纹肌溶解症的影响。 尤其是ICU停留时间长的患者肌肉量减少是导致sCr值与实际测量的肌酐清除率之间存在显著偏差的原因。
Full recovery from AKI is generally defned as the return of serum creatinine (sCr) below the threshold of AKI according to the KDIGO criteria. This defnition has important limitations. Baseline sCr is required to distinguish non-recovery from pre-existing chronic kidney disease. Most recent sCr preceeding acute illness or its back-calculation with formulas can be inaccurate. SCr at ICU admission is frequently altered by the dilution effect of volume resuscitation. Tubular secretion of creatinine, also afected by drugs, may contribute to the overestimation of glomerular fltration rate. Most importantly, SCr is infuenced by muscle mass and protein intake, liver disease, and rhabdomyolysis. Muscle mass frequently decreases, especially in patients with prolonged ICU stay, and causes a signifcant bias between sCr values and actual measured creatinine clearance.
-
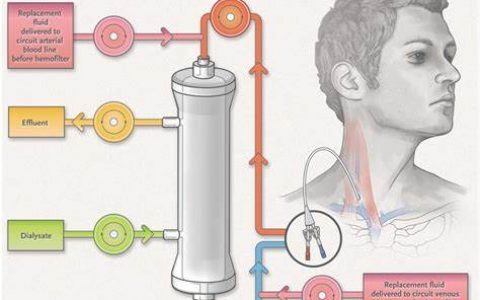
误解:急RRT治疗的高血流量会导致血流动力学不稳定(High blood flow rates in extracorporeal therapies cause hemodynamic instability)
体外治疗(ET)可能以不同方式影响血流动力学。 用患者血液灌注体外回路可致相对血容量不足。净超滤率超过血管内反流率导致血容量不足。 ET中的血管活性药物稀释/去除可能降低血清浓度和治疗效果。 间歇性血液透析过程中血液渗透压的突然下降已被证明是血液动力学恶化的危险因素。 由于血液在静脉 – 静脉闭合回路中运行,因此血流速不会造成血液动力学不稳定。 在稳定状态下,机器抽吸的血液量在同一时间单位内已回输给患者。
Extracorporeal therapies (ET) may impact hemodynamics in different ways. Priming the extracorporeal circuit with patient’s blood without reinfusing the priming solution causes a relative hypovolemia. Net ultrafltration rate exceeding the rate of intravascular reflling leads to hypovolemia. Vasoactive drugs dilution/removal during ET may decrease serum concentration and therapeutic efect. Sudden decrease in blood osmolality during intermittent hemodialysis has been shown to be a risk factor for hemodynamic worsening. Blood fow rate is never responsible for hemodynamic instability since blood runs in a veno-venous closed circuit. At steady state, the amount of blood withdrawn by the machine is reinfused to the patient in the same time unit.
-
误解:急颈静脉是肾脏替代治疗的最佳血管入路(Jugular vein is the best access for renal replacement therapy)
根据KDIGO指南,右侧颈内静脉(IJV)应该是肾替代治疗(RRT)的首选血管通路。右侧IJV的导管可直接进入右侧头臂静脉和上腔-右心房连接处,可能具有最好的流变性能。 定位在左侧IJV的导管可能具有弯曲的形状,并且需要更长的时间才能到达右心房:流速性能(特别是当从左头臂静脉抽血时)可能是不适当的。 然而,床边实践和一些现有文献认为,在非肥胖患者中,RRT的股动脉插管在感染,功能障碍或副作用方面可能类似于右侧IJV。
According to KDIGO guidelines, the right internal jugular vein (IJV) should be the frst-choice access for renal replacement therapy (RRT) . Catheters in the right IJV have a straight short course into the right brachiocephalic vein and cavo-atrial junction, likely allowing the best rheological performance. Catheters positioned in the left IJV may have a curved shape and they need to be longer to reach the right atrium: the flow performance (especially when blood is drawn from left brachiocephalic vein) might be inadequate. However, bedside practice and some available literature suggest that, in non-obese patients,femoral cannulation for RRT could be similar to right IJV in terms of infection, dysfunction, or side effects.
-
误解:急体外治疗中滤过即剂量(Effluent equals ET dose)
当小溶质的筛分系数等于1,并且在透析过程中发生透析液完全饱和时,滤过率等于治疗剂量(或清除率(K)),这在后稀释连续静脉 – 静脉血液滤过和持续低流速静脉 – 静脉血液透析是如此的。在所有其他情况下(间歇性血液透析或缓慢延长透析,预稀释血液滤过或血液透析滤过)和分子量高于500 Da的溶质,则该论断不正确,滤过率可能高估输送剂量。 此外,RRT剂量的概念应该包括“瞬时K”和应用有效时间。实际上,根据滤过率制定略高的RRT剂量(即30ml/kg/h)量,患者所需的目标剂量(即20ml/kg/h)完全能够达到。
When a small solute’s sieving coeffcient equals 1, and full saturation of dialysate occurs during dialysis, the effluent flow equals treatment dose (or clearance (K)) only in case of post-dilution continuous veno-venous hemofltration and low flow continuous veno-venous hemodialysis. In all other cases (intermittent hemodialysis or slow extended dialysis, predilution hemofltration, or hemodiafltration) and for solutes with molecular weight higher than 500 Da the statement is incorrect and effluent rate may overestimate delivered dose. Furthermore, the concept of RRT dose should include both “instantaneous K” and the effective time in which this is applied. Downtime may in fact create a mismatch between prescribed and delivered treatment dose.Hence, by slightly overprescribing the RRT dose based on effluent fow rate (i.e., 30 ml/kg/h), the target dose actually delivered to the patient (i.e., 20 ml/kg/h) can be reliably achieved.
-
误解:急RRT是脓毒症的“灵方”( ET is a “cure” for sepsis)
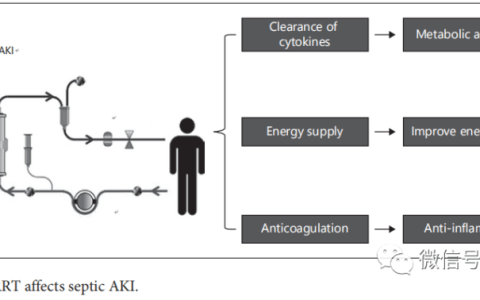
尽管有一些积极的实验观察,但没有临床试验显示ET对脓毒症和多器官功能衰竭患者死亡率的显著影响。内环境中的“坏”溶质(介质,细胞因子等)祛除是各种ET的基础。然而,病原体,宿主及其相互作用的巨大异质性可能是在普通人群中找到有效ET的困难之处。不同的技术应该根据精准医学的范畴确定特定的患者。但是,除内毒素外,ET祛除介质的机制仍然完全不明确。不经选择地祛除介质(可能是好的或不好的)的不利影响仍然没有得到足够的研究。ET只能被认为是影响脓毒症免疫系统的“辅助治疗”,而抗生素治疗和感染源控制仍然是脓毒症治疗的主流。控制酸中毒和液体平衡可能是ET治疗脓毒症无尿患者的主要临床目的,在感染源未控制的情况下最有效的ET将永远不会有效。
In spite of several positive experimental observations, no clinical trials have shown signifcant effects of ET on mortality in patients with sepsis and multiple organ failure. The rational to remove “bad” solutes (mediators, cytokines, etc.) restoring the milieu intérieur is the basis for a variety of ET. The vast heterogeneity of pathogens, hosts, and their interaction may, however, explain the difficulty to find an effective ET in the general population. Different techniques should be adapted to specific patients along the lines of precision medicine. However, with the exception of endotoxin, removal of mediators by ET is still completely unspecifc. The adverse effects of unselective removal of mediators (which may be good or bad) are still insuffciently investigated. While ET can only be considered “adjunctive therapies” aiming to affect the immune system during sepsis, antibiotic therapy and infection’s source control remain the mainstay of sepsis treatment. The control of acidosis and fluid balance are probably the main clinical targets when ET are prescribed to septic patients with anuria. The most effective ET will never be effective in the presence of an uncontrolled source of infection
-
误解:急我准备给无尿患者撤离RRT了——就停止治疗,补液并且上点大剂量襻利尿剂( I want to wean my anuric patient from RRT: let’s stop the treatment, give volume, and administer a big bolus of loop diuretic)
当由RRT支持的严重AKI的危重多器官功能障碍患者病情改善时(例如,不再需要血管加压支持和机械通气,并且体温和化验正常化)时,无尿仍然可能持续。由于尚无有效的撤机规程,而且AKI进展为慢性肾病评估仍是一个主要问题,因此在临床实践中可常可看到“强制”恢复尿量的尝试。事实上,肾脏并没有一个特定的“恢复截止期”,也没有可行的治疗策略。唯一可反向与ICU RRT成功撤离有关联的变量就是自主尿量的恢复(透析治疗过程中在没有利尿剂治疗情况下尿量≥400毫升/天,RRT停止12小时内的2小时肌酐清除率>23ml / min,24小时尿肌酐排泄(尽管利尿剂使用)至少5.2mmol。对RRT撤机仍需要进一步的前瞻性研究。
When the multiple organ dysfunction of a critically ill patient with severe AKI supported by ET improves (e.g., vasopressor support and mechanical ventilation are not needed anymore, and temperature and laboratory analyses are normalized), anuria may still be persistent. Since effective dialysis weaning protocols have never been described and concern about the evolution of AKI into a chronic renal condition is a major question, several attempts to “force” restoration of urine output can be seen in clinical practice. As a matter of fact, there is not a specifc “deadline” for the kidneys to recover and no available therapeutic strategy. The only variables retrospectively associated with successful interruption of ET in the ICU are the recovery of a spontaneous urine volume (during dialytic treatment) above 400 ml/day in the absence of diuretic therapy, a 2-h creatinine clearance within 12 h of RRT cessation above 23 ml/min, and 24 h urinary creatinine excretion (despite diuretic use) of at least 5.2mmol. Further prospective studies should be conducted in RRT weaning.

本文荟萃自公众号:“危通社” 微信公众号id:Newsccm,只做学术交流学习使用,不做为临床指导,本文观点不代表数字重症 ICU.CN立场。
 微信扫一扫
微信扫一扫