1 | SUMMARY OF WHAT IS NEW OR DIFFERENT
Changes to previous recommendations include:
-
诊断糖尿病酮症酸中毒(DKA)的生化标准纳入血清碳酸氢盐< 18 mmol/L
Biochemical criteria to diagnose diabetic ketoacidosis (DKA) include serum bicarbonate <18 mmol/L
-
在20–30分钟内输注初始液体大剂量
Infusion of initial fluid bolus(es) over 20–30 min
-
不再认为有必要在DKA治疗期间促进血清钠浓度升高
Promoting a rise in serum sodium concentrations during DKA treatment is no longer considered necessary
-
与标准DKA治疗相比,更加强调HHS治疗建议以及DKA和HHS(高渗性DKA)的混合表现的差异
Increased emphasis on differences in treatment recommendation for HHS and mixed presentation of DKA and HHS (hyperosmolar DKA) compared to standard DKA treatment
2 | EXECUTIVE SUMMARY
The biochemical criteria for the diagnosis of DKA are:
-
高血糖(血糖> 11 mmol/L [≈200 mg/dl])
Hyperglycemia (blood glucose >11 mmol/L [≈200 mg/dl])
-
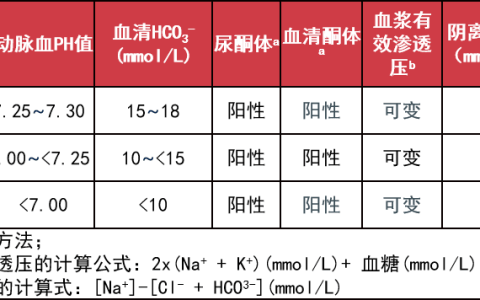
静脉pH <7.3或血清碳酸氢盐< 18 mmol/L(C)
Venous pH <7.3 or serum bicarbonate <18 mmol/L(C)
-
酮血症(血β-羟丁酸≥3 mmol/L) (C)或中量或大量酮尿。
Ketonemia (blood ß-hydroxybuyrate ≥3 mmol/L) (C) or moderate or large ketonuria.
Not all children or caregivers volunteer classic symptoms of diabetes (polyuria, polydipsia) at the time of diagnosis of DKA, and other symptoms of DKA are non-specific. Therefore, fingerstick blood glu-cose measurements should be considered for all children presenting with rapid breathing or with vomiting and abdominal pain without diarrhea.
The following recommendations are based on currently available evidence and are intended to be a general guide to DKA management. Because there is considerable individual variability in presentation of DKA (ranging from mild to severe and life threatening), some children may require specific treatment that, in the judgment of the treating physician, may occasionally be outside the range of options presented here. Clinical judgment should be used to determine optimal treat-ment for the individual child, and timely adjustments to treatment should be based on ongoing clinical and biochemical monitoring of the response to treatment.
Emergency assessment should follow the general guidelines for Pediatric Advanced Life Support(PALS) and includes:
-
立即检测血糖、血液或尿酮、血清电解质和血气;以及意识水平评估。(E)
Immediate mea-surement of blood glucose, blood or urine ketones, serum electrolytes and blood gases assessment of level of consciousness. (E)
-
建立静脉通道:两条外周静脉(IV)导管(E)。
-
Two peripheral intravenous (IV) catheters should be inserted (E)
Management should be conducted in a center experienced in the treatment of DKA in children and where vital signs, neurologi-cal status, and laboratory results can be monitored frequently.(E) Where geographic constraints require that management be initi-ated in a center with less experience, there should be telephone or videoconference support from a physician with expertise in DKA (E).
Meticulous monitoring of the clinical and biochemical response to treatment is necessary so that timely adjustments in treatment can be made when indicated by clinical or laboratory data (E).
Goals of therapy are to correct dehydration, correct acidosis and reverse ketosis, gradually restore hyperosmolality and blood glucose concentration to near normal, monitor for acute complications, and identify and treat any precipitating event.
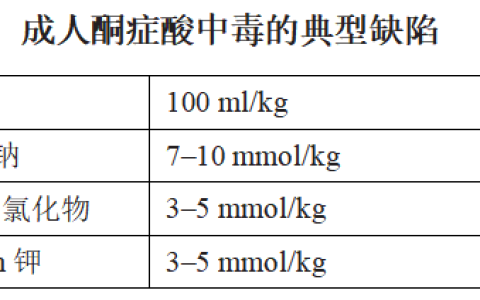
Fluid replacement should begin before starting insulin therapy. Expand volume using one or more boluses of 0.9% saline infused over 20–30 min to restore peripheral circulation (E). Calculate the subse-quent rate of fluid administration (0.45% to 0.9% saline), including the provision of maintenance fluid requirements, aiming to replace the estimated fluid deficit over 24 to 48 h (A).
Insulin therapy: begin with 0.05–0.1 U/kg/h (0.05 U/kg/h can be considered with pH > 7.15) at least 1 h AFTER starting fluid replace-ment therapy (B).
Potassium: If the child has hyperkalemia (potassium >5.5 mmol/L), defer potassium replacement therapy until urine out-put is documented. Begin intravenous fluid treatment with non-potassium containing fluids and measure potassium hourly. Begin potassium infusion when potassium <5.5 mmol/L. In the rare child with hypokalemia (potassium <3.0 mmol/L), defer insulin treatment and give a bolus of potassium (not to exceed 0.5 mEq/Kg/h), along with cardiac monitoring. Otherwise, begin with 40 mmol potas-sium/L (E).
Bicarbonate administration is not recommended except for treat-ment of life-threatening hyperkalemia or for severe acidosis (venous pH < 6.9) with evidence of compromised cardiac contractility (C).
Warning signs and symptoms of cerebral injury include: Onset of headache or vomiting after beginning treatment or progressively worsening or severe headache, slowing of heart rate not related to sleep or improved intravascular volume, change in neurological status (irritability, lethargy, confusion, incontinence), specific neurological signs (e.g., cranial nerve palsies), decreased oxygen saturation.(C) Hypertension occurs commonly in children with DKA and should not be considered a warning sign for cerebral injury, in the absence of other findings.
In children with multiple risk factors for cerebral injury (elevated serum urea nitrogen concentration (>20 mg/dl), severe acidosis (pH < 7.1), severe hypocapnia (pCO2 < 21 mmHg), age < 5 years), have mannitol or hypertonic saline at the bedside and the dose calcu-lated. (E) If neurologic status deteriorates acutely, hyperosmolar ther-apy with mannitol or hypertonic saline should be given immediately (C).
Prevention: Management of DKA is not complete until an attempt has been made to identify and treat the cause.
-
在已知糖尿病无既往疾病的儿童中,DKA几乎总是未能适当地进行胰岛素注射或中断胰岛素输送的结果,最常见的原因是胰岛素泵输入装置功能障碍。
DKA without a preceding illness in a child with known diabetes is almost always the result of failure to appropriately administer insulin injections or inter-ruption of insulin delivery, most often as a result of insulin pump infu-sion set dysfunction. In new onset diabetes
-
在新发糖尿病中,DKA常常是诊断延迟的结果(E)。
DKA is frequently the consequence of a delay in diagnosis (E).
The criteria for Hyperglycemic Hyperosmolar State (HHS) include all the following:
-
血浆葡萄糖浓度> 33.3 mmol/L (600 mg/dl)
Plasma glucose concentration > 33.3 mmol/L (600 mg/dl)
-
静脉pH > 7.25动脉pH > 7.30
Venous pH > 7.25; arterial pH > 7.30
-
血清碳酸氢盐> 15 mmol/L
Serum bicarbonate >15 mmol/L
-
较轻的酮尿症,无至轻度酮血症
Small ketonuria, absent to mild ketonemia
-
有效血清渗透压> 320 mOsm/kg
Effective serum osmolality >320 mOsm/kg
在HHS,初始液体治疗的目标是血管内和血管外扩容,恢复正常肾灌注,并促进校正后的血清钠浓度和血清渗透压逐渐下降。HHS和DKA在治疗策略上的差异包括给药液体量、胰岛素给药时间以及监测校正后血清钠浓度下降。
In HHS, the goals of initial fluid therapy are to expand the intra-and extravascular volume, restore normal renal perfusion, and pro-mote a gradual decline in corrected serum sodium concentration and serum osmolality. Differences in treatment strategy between HHS and DKA include the volume of fluid administered, the timing of insulin administration, and monitoring of the decline in corrected serum sodium concentration.
In HHS, begin insulin administration at a dose of 0.025 to 0.05 U/kg/h once plasma glucose is decreasing less than 3 mmol/L (50 mg/dl) per hour with fluid alone (C). Rates of fluid administration, both as initial fluid boluses to restore circulation and as ongoing defi-cit replacement, are substantially higher than for DKA.
本文荟萃自,只做学术交流学习使用,不做为临床指导,本文观点不代表数字重症 ICU.CN立场。
 微信扫一扫
微信扫一扫