Sepsis-associated acute kidney injury in the intensive care unit: incidence, patient characteristics, timing, trajectory, treatment, and associated outcomes. A multicenter,
observational study
ICM:脓毒症相关急性肾损伤:发病率、患者特征、时间、轨迹、治疗和相关结局;一项多中心、观察性研究
文章来源:doi.org/10.1007/s00134-023-07138-0


Purpose
The Acute Disease Quality Initiative (ADQI) Workgroup recently released a consensus defnition of sepsisassociated acute kidney injury (SA-AKI), combining Sepsis-3 and Kidney Disease Improving Global Outcomes (KDIGO) AKI criteria. This study aims to describe the epidemiology of SA-AKI.
目的
急性疾病质量倡议(ADQI)工作组最近发布了脓毒症相关急性肾损伤(SA-AKI)的共识定义,结合sepsis-3和肾病改善全球结局(KDIGO)AKI标准。本研究旨在描述SA-AKI的流行病学。
Methods
This is a retrospective cohort study carried out in 12 intensive care units (ICUs) from 2015 to 2021. We studied the incidence, patient characteristics, timing, trajectory, treatment, and associated outcomes of SA-AKI based on the ADQI defnition.
方法
这是一项回顾性队列研究,于2015年至2021年在12个重症监护室(ICU)进行。我们研究了基于ADQI定义的SA-AKI的发病率、患者特征、时间、轨迹、治疗和相关结局。



Results
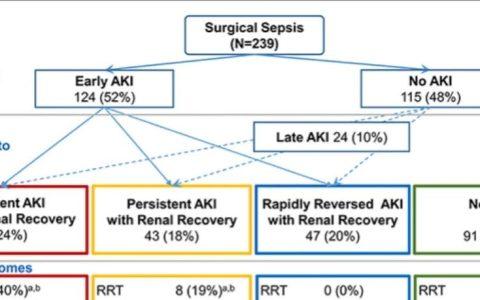
Out of 84,528 admissions, 13,451 met the SA-AKI criteria with its incidence peaking at 18% in 2021. SA-AKI patients were typically admitted from home via the emergency department (ED) with a median time to SA-AKI diagnosis of 1 day (interquartile range (IQR) 1–1) from ICU admission. At diagnosis, most SA-AKI patients (54%) had a stage 1 AKI, mostly due to the low urinary output (UO) criterion only (65%). Compared to diagnosis by creatinine alone, or by both UO and creatinine criteria, patients diagnosed by UO alone had lower renal replacement therapy (RRT) requirements (2.8% vs 18% vs 50%; p<0.001), which was consistent across all stages of AKI. SA-AKI hospital mortality was 18% and SA-AKI was independently associated with increased mortality. In SA-AKI, diagnosis by low UO only, compared to creatinine alone or to both UO and creatinine criteria, carried an odds ratio of 0.34 (95% confdence interval (CI) 0.32–0.36) for mortality.
结果
在84,528名入院者中,有13,451人符合SA-AKI标准,其发病率在2021年达到18%的峰值。SA-AKI患者通常通过急诊科(ED)入院,从ICU入院至SA-AKI诊断的中位时间为1天(四分位距(IQR)1-1)。在诊断时,大多数SA-AKI患者(54%)患有1期AKI,主要是由于低尿量(UO)标准(65%)。与单独通过肌酐诊断或通过UO和肌酐标准诊断相比,单独通过UO诊断的患者的肾脏替代治疗(RRT)需求较低(2.8% vs 18% vs 50%; p<0.001),这在AKI的所有分期中一致。SA-AKI住院死亡率为18%,SA-AKI与死亡率增加独立相关。在SA-AKI中,仅通过低UO诊断,与单独的肌酐或UO和肌酐标准相比,死亡率的比值比为0.34(95%置信区间(CI)0.32-0.36)。



Conclusions
SA-AKI occurs in 1 in 6 ICU patients, is diagnosed on day 1 and carries signifcant morbidity and mortality risk with patients mostly admitted from home via the ED. However, most SA-AKI is stage 1 and mostly due to low UO, which carries much lower risk than diagnosis by other criteria.
结论
SA-AKI发生在1/6的ICU患者中,在第1天被诊断,并且绝大多数患者通过急诊科入院,具有显著的发病率和死亡率风险。然而,大多数SA-AKI是1期,主要是由于低UO,其风险比其他标准诊断低得多。
Strengths and limitations
Our study had several strengths. First, it was conducted on a large cohort with a wide array of ICU admissions from a state-wide ICU system encompassing a complete range of adult critical care. Tis population is representative of the general Australian population and likely representative of similar populations in resource-rich countries. Second, our study data were comprehensive with highly granular data, which was electronically extracted from a ubiquitous clinical information system. All data collected were clinically validated and had minimal missing data points. Moreover, given their collection by non-research staf, they represent an unbiased sample. Tird, although we utilised a novel standardised defnition for SA-AKI, the defnition is composed of the SEPSIS-3 and KDIGO AKI defnitions, which are well established in the literature. As such, we were able to leverage well-recognised techniques to analyse a large database to identify sepsis and AKI.
We acknowledge some limitations. First, the detection of sepsis and AKI, and therefore, SA-AKI, was done electronically and patients may have been misclassifed. Organ dysfunction detected by the analysis may not have been caused by infection. However, our very large cohort of patients likely limits the impact of these unusual circumstances. Second, we did not classify SA-AKI into phenotypes as suggested by the ADQI 28 Workgroup. Tus, our cohort of SA-AKI patients may represent different groups with diverging risk factors and outcomes. We plan to focus future work on such phenotypes. Tird, as we could not identify which patients had CKD before presentation, such patients would have led to an overestimation of AKI when using estimated baseline creatinine calculation. Tis matters, because CKD patients have specifc features and diferent outcomes from those without CKD. However, a previous study in investigated over 3500 of the same patients from four hospitals involved in this study, and using diferent data reported a low CKD prevalence of 13.5%. Investigation of CKD patients will require additional data acquisition in future studies. Fourth, the censoring of an RRT and serum creatinine components of MAKE-30 at discharge from the ICU potentially introduced ascertainment bias. Lastly, the imputation of hourly UO data could potentially misclassify patients with AKI. However, the sensitivity analysis demonstrates no systemic diferences between groups and reduction, not increase, in AKI diagnoses with imputation.
优势与局限性
优点:1.是在一个大型队列中进行的,该队列来自全州范围内的ICU系统,包括完整的成人重症监护。它的人口代表了澳大利亚的一般人口,也可能代表了资源丰富国家的类似人口。2.研究数据是全面的,具有高度颗粒化的数据,这些数据是从无处不在的临床信息系统中以电子方式提取的。收集的所有数据均经过临床验证,缺失数据点极少。此外,考虑到它们是由非研究人员收集的,它们代表了一个无偏见的样本。3.尽管使用了SA-AKI的新标准化定义,但该定义由文献中已确立的SEPSIS-3和KDIGO AKI定义组成。因此,我们能够利用公认的技术来分析大型数据库,以识别脓毒症和AKI。
局限性:1.脓毒症和AKI的检测,以及SA-AKI的检测,是以电子方式进行的,患者可能被错误分类。通过分析检测到的器官功能障碍可能不是由感染引起的。然而,我们非常大的患者队列可能会限制这些异常情况的影响。2.我们没有按照ADQI 28工作组的建议将SA-AKI分为表型。因此,我们的SA-AKI患者队列可能代表了具有不同风险因素和结局的不同人群。我们计划将未来的工作重点放在这些表型上。3.由于我们无法确定哪些患者在就诊前患有CKD,因此当使用估计的基线肌酐计算时,这些患者会导致AKI的高估。这很重要,因为CKD患者与非CKD患者有特定的特征和不同的结局。然而,先前的一项研究调查了来自参与本研究的四家医院的3500多名相同患者,并使用不同的数据报告了13.5%的低CKD患病率。在未来的研究中,CKD患者的研究将需要额外的数据采集。4.从ICU出院时对RRT和MAKE-30的血清肌酐组分进行删失可能会引入确定偏倚。5.每小时UO数据的插补可能会对AKI患者进行错误分类。然而,敏感性分析表明,两组之间没有系统性差异,AKI诊断的插补减少而不是增加。
本文荟萃自公众号:IE-learning IElearning急危重症学习平台,只做学术交流学习使用,不做为临床指导,本文观点不代表数字重症 ICU.CN立场。
 微信扫一扫
微信扫一扫